Laurie's Blogs.

Apr 2024
Neurorehabilitation for dogs with spinal shock in severe spinal cord injuries
I get giddy when I come across fantastically pivotal research just by happenstance! Here’s one of those papers.
Gouveia D, Carvalho C, Vong N, et al. Spinal shock in severe SCI dogs and early implementation of intensive neurorehabilitation programs. Res Vet Sci. 2023 Nov;164:105018. https://pubmed.ncbi.nlm.nih.gov/37722219/
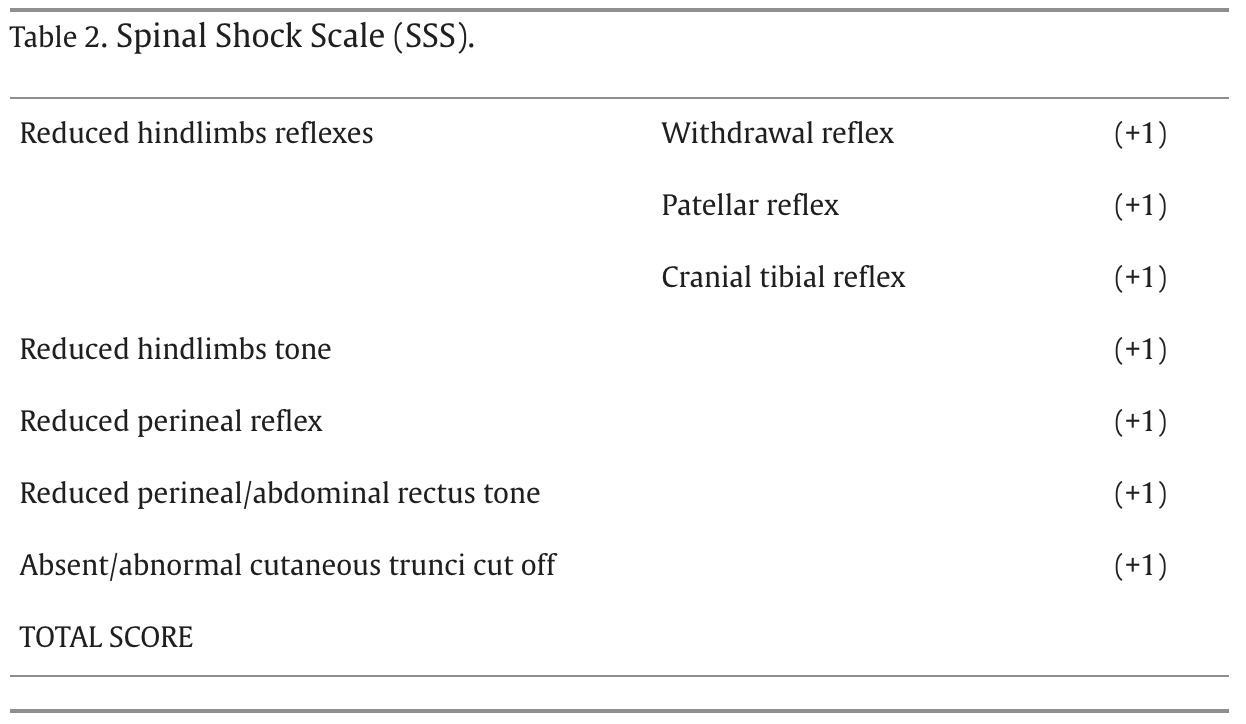
Firstly, what is Spinal Shock?
“Spinal shock syndrome is still not widely described in veterinary medicine and may be explained as an evident depression in the segmental spinal reflexes with loss of muscle tone caudally to the spinal cord injury (SCI), despite remaining physically intact local reflex arcs. There is also the possibility of fecal and urinary incontinence and usually this transient hyporeflexia or areflexia progresses to possible hyperreflexia within days to months ”
“In human medicine, it has been described a 4-phase model, which comprises phase 1 (0-24 h) based in the areflexia/hyporeflexia caudal to the lesion, phase 2 (1–3 days) when reflexes start to return characterized by denervation supersensitivity and receptor upregulation, phase 3 (1–4 weeks) with early hyperreflexia and new synapses growth and phase 4 (1–12 months) described by late hyperreflexia.”
“This prospective controlled blinded cohort study aims to understand the implication of spinal shock in neurorehabilitation of severe SCI dogs and the importance of its evaluation thought a spinal shock scale (SSS).”
Methods:
371 dogs were recruited for this prospective study that collected data between 2017 and 2023. All had severe SCI due to compressive T3-L3 myelopathy (Hansen type I and type II) or non-compressive myelopathy (ANNPE and FCE) and all had to be admitted in the centers until a maximum of 72 h after injury, with or without surgical approach.
Dogs with signs of spinal shock (n = 245) were allocated in the study group (SG) and dogs without these signs (n = 126) in the control group (CG). The SSS, a punctuation scale (0–7), was evaluated at admission and each 6 h for 3 days, each day for 15 days, each week for 6 weeks, each month until 3 months, followed by 3 monthly follow-ups.
(For more of the nitpicky aspects of methods, please click on the link to the abstract and then to the open access article.)
REHAB:
See Table 3 from the paper
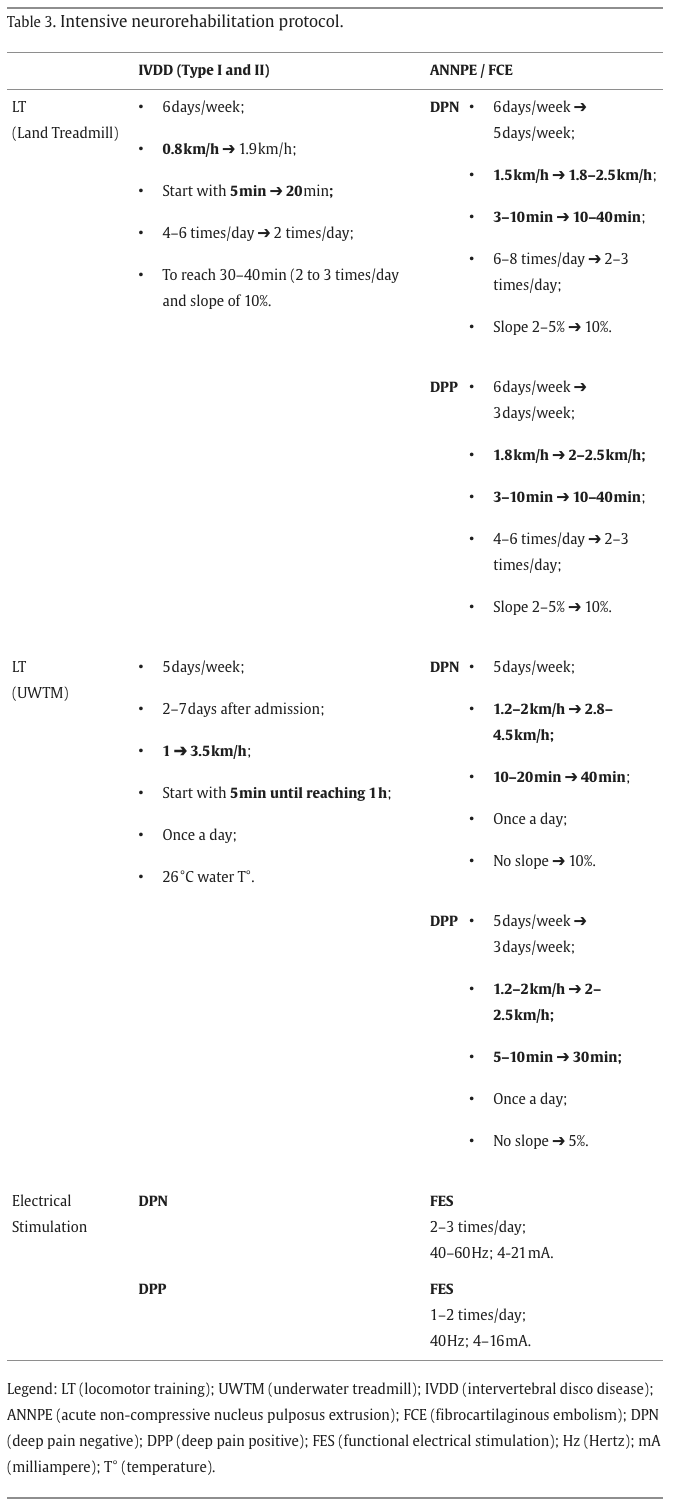
Dogs from both groups underwent an intensive neurorehabilitation protocol, according to each etiology (IVDD, ANNPE and FCE), which included locomotor training, functional electrical stimulation (FES) programs and other rehabilitation modalities and methods.
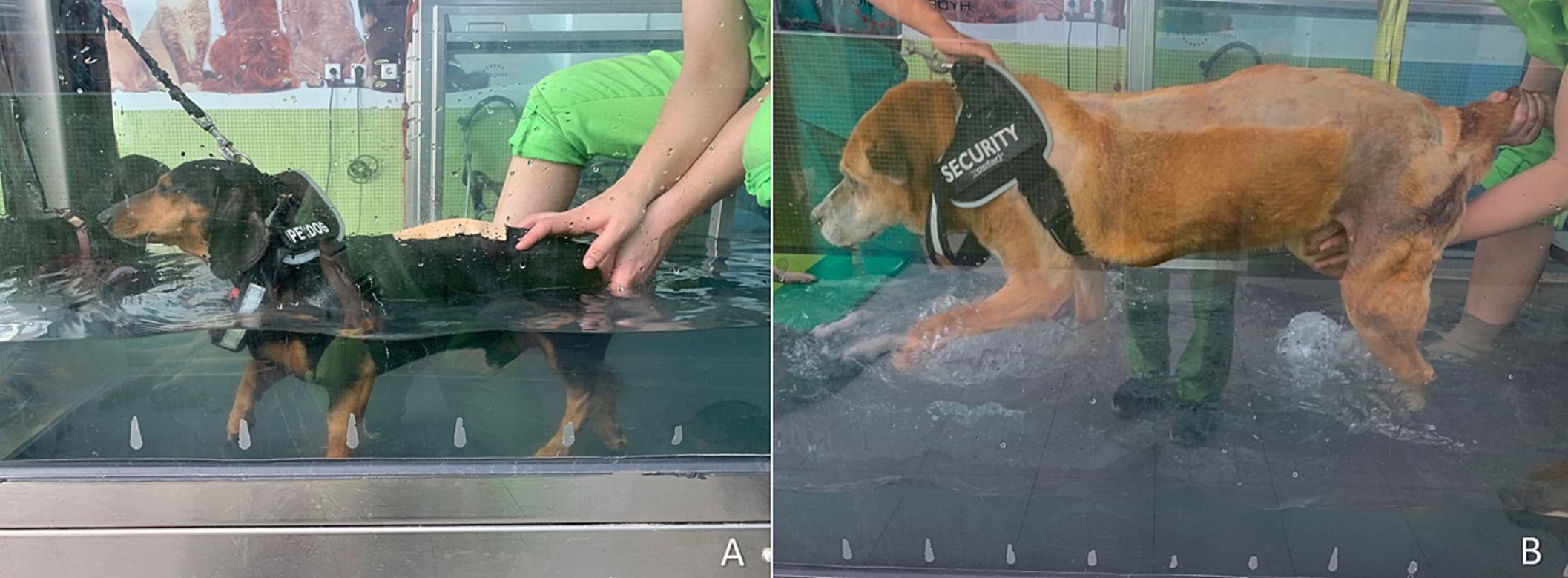

In addition to UWT / TM training, all dogs engaged in kinesiotherapy exercises, however with different degrees of difficulty regarding muscle contraction, voluntary or automatic, according to each patient condition. Standard evolution begun with passive exercises, progressing to active assisted and finally active exercises.
Stimulation of postural standing, flexor exercises and bicycle movements (always standing if possible) were examples of passive exercises, while body weight supported stimulation of the gait, alternated floor types and cavaletti rails were considered active assisted exercises. In dogs with manifestation of muscle hypotonicity, bicycle movements and flexor exercises had to be performed with limb stretching.
When patients were able to perform these exercises without body weight support, they were considered active exercises, in addition with balance board postural standing, vertical poles exercises and up-downs ramps. Time for these exercises was the same with 10 min repetitions, two to four times a day.
Dogs that presented muscle trigger points were subjected to class IV laser therapy (Companion Therapy Laser ®) for pain control: 12 J/cm2, 2,5 Hz, duty cycle 88%, 3 min, pulsed mode. This modality was also applied in dogs with pressure sores but to accelerate healing, as followed: 2 W, 30 s, each time at 20 Hz, 500 Hz, 5000 Hz and 10,000 Hz, in this specific order.
Findings:
Dogs that were admitted after 72 h and maintained SSS ≥ 4 were fewer and none recovered ambulation, not agreeing with the expectable evolution and resulting in a worse prognosis. The long-term signs are usually associated with decrease of withdrawal reflex accompanied by changes in the fusimotor tone due to the lack of input in hindlimbs lower motor neurons (LMN) by the pathways located at the ventral and lateral funiculi, essentially the rubrospinal, vestibulospinal and reticulospinal, which contributes for the spinal shock development and progression.
The study group (spinal shock group) discharged 66.9% ambulatory dogs versus 97.6% of control dogs.
Mean time to ambulation was 31.57 days for the spinal shock group and 23.02 days for the control group for the total of the 287 ambulatory dogs.
Within the study group, deep pain confirmed to be a prognosis factor for ambulation and only deep pain negative (DPN) dogs that recovered deep pain could achieve an ambulatory status.
There was no case of spinal reflex locomotion in the study group, contrary to the control group with DPN dogs achieving ambulation without deep pain recovery but most of them needing 90 days of rehabilitation
Furthermore, this study revealed a total of 5.7% of myelomalacia cases with a slight increase in the study group with 7.3% (18/245) and 7 dogs diagnosed with progressive myelomalacia.
Important Conclusions
Neurorehabilitation intends to promote sprouting and synapse's function formation from spared descending motor axons aiming to stimulate central pattern generators (CPGs) and improve the interneurons network to achieve stereotypic multi-joints rhythmic alternating movements needed for stepping.
For neurorehabilitation, the enthusiastic idea would be the possibility to work with those spinal shock patients diagnosed with severe SCI, in a synergic way between neurology and neurorehabilitation, ideally in early hyperacute phase after injury.
Laurie’s thoughts:
Well, I can sum it up quite simply, get these neurological / spinal shock dogs in for intensive rehabilitation asap.
That’s it!
Until next time, Cheers!
Laurie
